 Login / Register
Login / Register 



- Clone
- RPA-T4 (See other available formats)
- Regulatory Status
- RUO
- Workshop
- IV T114
- Other Names
- T4
- Isotype
- Mouse IgG1, κ
- Ave. Rating
- Submit a Review
- Product Citations
- publications

-

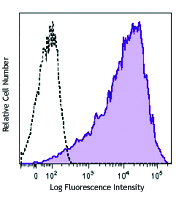
Human peripheral blood lymphocytes stained with RPA-T4 FITC -

Confocal image of human lymph node sample acquired using the IBEX method of highly multiplexed antibody-based imaging: CD163 (red) in Cycle 3 and CD4 (blue) in Cycle 5. Tissues were prepared using ~1% (vol/vol) formaldehyde and a detergent. Following fixation, samples are immersed in 30% (wt/vol) sucrose for cryoprotection. Images are courtesy of Drs. Andrea J. Radtke and Ronald N. Germain of the Center for Advanced Tissue Imaging (CAT-I) in the National Institute of Allergy and Infectious Diseases (NIAID, NIH).
CD4, also known as T4, is a 55 kD single-chain type I transmembrane glycoprotein expressed on most thymocytes, a subset of T cells, and monocytes/macrophages. CD4, a member of the Ig superfamily, recognizes antigens associated with MHC class II molecules, and participates in cell-cell interactions, thymic differentiation, and signal transduction. CD4 acts as a primary receptor for HIV, binding to HIV gp120. CD4 has also been shown to interact with IL-16.
Product DetailsProduct Details
- Reactivity
- Human
- Antibody Type
- Monoclonal
- Host Species
- Mouse
- Formulation
- Phosphate-buffered solution, pH 7.2, containing 0.09% sodium azide and BSA (origin USA)
- Preparation
- The antibody was purified by affinity chromatography, and conjugated with FITC under optimal conditions.
- Concentration
- Lot-specific (to obtain lot-specific concentration and expiration, please enter the lot number in our Certificate of Analysis online tool.)
- Storage & Handling
- The CD4 antibody solution should be stored undiluted between 2°C and 8°C, and protected from prolonged exposure to light. Do not freeze.
- Application
-
FC - Quality tested
SB - Reported in the literature, not verified in house - Recommended Usage
-
Each lot of this antibody is quality control tested by immunofluorescent staining with flow cytometric analysis. For flow cytometric staining, the suggested use of this reagent is 5 µl per million cells in 100 µl staining volume or 5 µl per 100 µl of whole blood.
- Excitation Laser
-
Blue Laser (488 nm)
- Application Notes
-
The RPA-T4 antibody binds to the D1 domain of CD4 (CDR1 and CDR3 epitopes) and can block HIV gp120 binding and inhibit syncytia formation. Additional reported applications (for the relevant formats) include: immunohistochemistry of acetone-fixed frozen sections3,4,5, blocking of T cell activation1,2, and spatial biology (IBEX)10,11. This clone was tested in-house and does not work on formalin fixed paraffin-embedded (FFPE) tissue. The Ultra-LEAF™ purified antibody (Endotoxin < 0.01 EU/µg, Azide-Free, 0.2 µm filtered) is recommended for functional assays (Cat. No. 300569 - 300574).
- Additional Product Notes
-
Iterative Bleaching Extended multi-pleXity (IBEX) is a fluorescent imaging technique capable of highly-multiplexed spatial analysis. The method relies on cyclical bleaching of panels of fluorescent antibodies in order to image and analyze many markers over multiple cycles of staining, imaging, and, bleaching. It is a community-developed open-access method developed by the Center for Advanced Tissue Imaging (CAT-I) in the National Institute of Allergy and Infectious Diseases (NIAID, NIH).
- Application References
-
- Knapp W, et al. 1989. Leucocyte Typing IV. Oxford University Press. New York. (Activ)
- Moir S, et al. 1999. J. Virol. 73:7972. (Activ)
- Deng MC, et al. 1995. Circulation 91:1647. (IHC)
- Friedman T, et al. 1999. J. Immunol. 162:5256. (IHC)
- Mack CL, et al. 2004. Pediatr. Res. 56:79. (IHC)
- Lan RY, et al. 2006. Hepatology 43:729.
- Zenaro E, et al. 2009. J. Leukoc. Biol. 86:1393. (FC) PubMed
- Yoshino N, et al. 2000. Exp. Anim. (Tokyo) 49:97. (FC)
- Stoeckius M, et al. 2017. Nat. Methods. 14:865. (PG)
- Radtke AJ, et al. 2020. Proc Natl Acad Sci USA. 117:33455-33465. (SB) PubMed
- Radtke AJ, et al. 2022. Nat Protoc. 17:378-401. (SB) PubMed
- Product Citations
- RRID
-
AB_314073 (BioLegend Cat. No. 300505)
AB_314074 (BioLegend Cat. No. 300506)
AB_2562052 (BioLegend Cat. No. 300538)
Antigen Details
- Structure
- Ig superfamily, type I transmembrane glycoprotein, 55 kD
- Distribution
-
T cell subset, majority of thymocytes, monocytes/macrophages
- Function
- MHC class II co-receptor, lymphocyte adhesion, thymic differentiation, HIV receptor
- Ligand/Receptor
- MHC class II molecules, HIV gp120, IL-16
- Cell Type
- Dendritic cells, Macrophages, Monocytes, T cells, Thymocytes, Tregs
- Biology Area
- Immunology
- Molecular Family
- CD Molecules
- Antigen References
-
1. Center D, et al. 1996. Immunol. Today 17:476.
2. Gaubin M, et al. 1996. Eur. J. Clin. Chem. Clin. Biochem. 34:723. - Gene ID
- 920 View all products for this Gene ID
- UniProt
- View information about CD4 on UniProt.org
Related Pages & Pathways
Pathways







Related FAQs
- I am unable to see expression of T cell markers such as CD3 and CD4 post activation.
- TCR-CD3 complexes on the T-lymphocyte surface are rapidly downregulated upon activation with peptide-MHC complex, superantigen or cross-linking with anti-TCR or anti-CD3 antibodies. PMA/Ionomycin treatment has been shown to downregulate surface CD4 expression. Receptor downregulation is a common biological phenomenon and so make sure that your stimulation treatment is not causing it in your sample type.
- If an antibody clone has been previously successfully used in IBEX in one fluorescent format, will other antibody formats work as well?
-
It’s likely that other fluorophore conjugates to the same antibody clone will also be compatible with IBEX using the same sample fixation procedure. Ultimately a directly conjugated antibody’s utility in fluorescent imaging and IBEX may be specific to the sample and microscope being used in the experiment. Some antibody clone conjugates may perform better than others due to performance differences in non-specific binding, fluorophore brightness, and other biochemical properties unique to that conjugate.
- Will antibodies my lab is already using for fluorescent or chromogenic IHC work in IBEX?
-
Fundamentally, IBEX as a technique that works much in the same way as single antibody panels or single marker IF/IHC. If you’re already successfully using an antibody clone on a sample of interest, it is likely that clone will have utility in IBEX. It is expected some optimization and testing of different antibody fluorophore conjugates will be required to find a suitable format; however, legacy microscopy techniques like chromogenic IHC on fixed or frozen tissue is an excellent place to start looking for useful antibodies.
- Are other fluorophores compatible with IBEX?
-
Over 18 fluorescent formats have been screened for use in IBEX, however, it is likely that other fluorophores are able to be rapidly bleached in IBEX. If a fluorophore format is already suitable for your imaging platform it can be tested for compatibility in IBEX.
- The same antibody works in one tissue type but not another. What is happening?
-
Differences in tissue properties may impact both the ability of an antibody to bind its target specifically and impact the ability of a specific fluorophore conjugate to overcome the background fluorescent signal in a given tissue. Secondary stains, as well as testing multiple fluorescent conjugates of the same clone, may help to troubleshoot challenging targets or tissues. Using a reference control tissue may also give confidence in the specificity of your staining.
- How can I be sure the staining I’m seeing in my tissue is real?
-
In general, best practices for validating an antibody in traditional chromogenic or fluorescent IHC are applicable to IBEX. Please reference the Nature Methods review on antibody based multiplexed imaging for resources on validating antibodies for IBEX.
Customers Also Purchased


Compare Data Across All Formats
This data display is provided for general comparisons between formats.
Your actual data may vary due to variations in samples, target cells, instruments and their settings, staining conditions, and other factors.
If you need assistance with selecting the best format contact our expert technical support team.



Follow Us