


- Clone
- 9C4 (See other available formats)
- Regulatory Status
- RUO
- Other Names
- Ep-CAM, tumor associated calcium signal transducer 1, epithelial cell surface antigen, epithelial glycoprotein 2, EGP2, adenocarcinoma associated antigen, TROP1
- Isotype
- Mouse IgG2b, κ
- Ave. Rating
- Submit a Review
- Product Citations
- publications
9C4_Alx647_071007")
-
9C4_Alx647_071007")
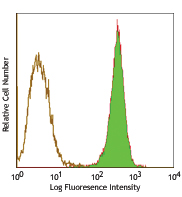
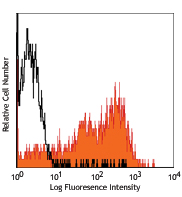
Human colon carcinoma cell line (HT29) stainined with 9C4 Alexa Fluor® 647 -

MCF7 breast cancer cell line was stained with 4 µg/mL anti-human CD326 Alexa Fluor® 647 and nuclear counterstained with DAPI. Images were acquired with a TE300 fluorescence microscope with a 20x objective. Data provided by: Er Liu and John Nolan, La Jolla Bioengineering Institute
| Cat # | Size | Price | Save |
|---|---|---|---|
| 324212 | 100 tests | ¥64,460 |
CD326 is also known as Ep-CAM, tumor associated calcium signal transducer 1, epithelial cell surface antigen, epithelial glycoprotein 2, EGP2, adenocarcinoma associated antigen, and TROP1. CD326 is a type I transmembrane protein containing six disulfide bridges and one THYRO domain. This cell surface glycosylated 40 kD protein is highly expressed in bone marrow, colon, lung, and most normal epithelial cells and is expressed on carcinomas of gastrointestinal origin. Recently, it has been reported that CD326 expression occurs during the early steps of erythrogenesis. CD326 functions as a homotypic calcium-independent cell adhesion molecule and is believed to be involved in carcinogenesis by its ability to induce genes involved in cellular metabolism and proliferation. CD326 antigen is an immunotherapeutic target for the treatment of human carcinomas.
Product DetailsProduct Details
- Reactivity
- Human
- Antibody Type
- Monoclonal
- Host Species
- Mouse
- Immunogen
- DU.4475 breast carcinoma
- Formulation
- Phosphate-buffered solution, pH 7.2, containing 0.09% sodium azide and BSA (origin USA)
- Preparation
- The antibody was purified by affinity chromatography and conjugated with Alexa Fluor® 647 under optimal conditions.
- Concentration
- Lot-specific (to obtain lot-specific concentration, please enter the lot number in our Concentration and Expiration Lookup or Certificate of Analysis online tools.)
- Storage & Handling
- The antibody solution should be stored undiluted between 2°C and 8°C, and protected from prolonged exposure to light. Do not freeze.
- Application
-
FC - Quality tested
ICC - Verified
SB - Reported in the literature, not verified in house - Recommended Usage
-
Each lot of this antibody is quality control tested by immunofluorescent staining with flow cytometric analysis. For flow cytometric staining, the suggested use of this reagent is 5 µL per million cells in 100 µL staining volume or 5 µL per 100 µL of whole blood. It is recommended that the reagent be titrated for optimal performance for each application.
* Alexa Fluor® 647 has a maximum emission of 668 nm when it is excited at 633nm / 635nm.
Alexa Fluor® and Pacific Blue™ are trademarks of Life Technologies Corporation.
View full statement regarding label licenses - Excitation Laser
-
Red Laser (633 nm)
- Application Notes
-
Additional reported applications (for the revelant formats) include: immunofluorescence, immunohistochemistry3, and spatial biology (IBEX)4,5.
- Additional Product Notes
-
Iterative Bleaching Extended multi-pleXity (IBEX) is a fluorescent imaging technique capable of highly-multiplexed spatial analysis. The method relies on cyclical bleaching of panels of fluorescent antibodies in order to image and analyze many markers over multiple cycles of staining, imaging, and, bleaching. It is a community-developed open-access method developed by the Center for Advanced Tissue Imaging (CAT-I) in the National Institute of Allergy and Infectious Diseases (NIAID, NIH).
-
Application References
(PubMed link indicates BioLegend citation) -
- Lammers R, et al. 2002. Exp. Hematol. 30:537.
- Schultz LD, et al. 2010. P. Natl. Acad. Sci. USA 107:13022. PubMed
- Human Protein Atlas http://www.proteinatlas.org/ENSG00000119888/antibody (IHC)
- Radtke AJ, et al. 2020. Proc Natl Acad Sci USA. 117:33455-33465. (SB) PubMed
- Radtke AJ, et al. 2022. Nat Protoc. 17:378-401. (SB) PubMed
- Product Citations
- RRID
-
AB_756086 (BioLegend Cat. No. 324212)
Antigen Details
- Structure
- Type I transmembrane protein, contains six disulfide bridges, one THYRO domain, approximate molecular weight 40 kD.
- Distribution
-
Highly expressed in bone marrow, colon, lung, and most normal epithelial cells. Also highly expressed on carcinomas of gastrointestinal origin. Expressed during early erythrogenesis.
- Function
- Homotypic calcium-independent cell adhesion. CD326 is believed to be involved in carcinogenesis by its ability to induce genes involved in cellular metabolism and proliferation.
- Modification
- Glycosylated.
- Cell Type
- Embryonic Stem Cells, Epithelial cells
- Biology Area
- Cell Biology, Immunology, Stem Cells
- Molecular Family
- Adhesion Molecules, CD Molecules
- Antigen References
-
1. Strnad J, et al. 1989. Cancer Res. 49:314.
2. Munz M, et al. 2004. Oncogene 23:5748.
3. Rao CG, et al. 2005. Int. J. Oncol. 27:49. - Gene ID
- 4072 View all products for this Gene ID
- UniProt
- View information about CD326 on UniProt.org







Related FAQs
- If an antibody clone has been previously successfully used in IBEX in one fluorescent format, will other antibody formats work as well?
-
It’s likely that other fluorophore conjugates to the same antibody clone will also be compatible with IBEX using the same sample fixation procedure. Ultimately a directly conjugated antibody’s utility in fluorescent imaging and IBEX may be specific to the sample and microscope being used in the experiment. Some antibody clone conjugates may perform better than others due to performance differences in non-specific binding, fluorophore brightness, and other biochemical properties unique to that conjugate.
- Will antibodies my lab is already using for fluorescent or chromogenic IHC work in IBEX?
-
Fundamentally, IBEX as a technique that works much in the same way as single antibody panels or single marker IF/IHC. If you’re already successfully using an antibody clone on a sample of interest, it is likely that clone will have utility in IBEX. It is expected some optimization and testing of different antibody fluorophore conjugates will be required to find a suitable format; however, legacy microscopy techniques like chromogenic IHC on fixed or frozen tissue is an excellent place to start looking for useful antibodies.
- Are other fluorophores compatible with IBEX?
-
Over 18 fluorescent formats have been screened for use in IBEX, however, it is likely that other fluorophores are able to be rapidly bleached in IBEX. If a fluorophore format is already suitable for your imaging platform it can be tested for compatibility in IBEX.
- The same antibody works in one tissue type but not another. What is happening?
-
Differences in tissue properties may impact both the ability of an antibody to bind its target specifically and impact the ability of a specific fluorophore conjugate to overcome the background fluorescent signal in a given tissue. Secondary stains, as well as testing multiple fluorescent conjugates of the same clone, may help to troubleshoot challenging targets or tissues. Using a reference control tissue may also give confidence in the specificity of your staining.
- How can I be sure the staining I’m seeing in my tissue is real?
-
In general, best practices for validating an antibody in traditional chromogenic or fluorescent IHC are applicable to IBEX. Please reference the Nature Methods review on antibody based multiplexed imaging for resources on validating antibodies for IBEX.
Customers Also Purchased

Compare Data Across All Formats
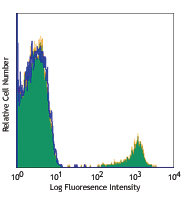
This data display is provided for general comparisons between formats.
Your actual data may vary due to variations in samples, target cells, instruments and their settings, staining conditions, and other factors.
If you need assistance with selecting the best format contact our expert technical support team.



Follow Us